Most tablets and capsules taken by mouth enter the stomach and dissolve there, before entering the small intestine for absorption. On the other hand, enteric-coated tablets are designed with a special coating to allow the medication to pass through the acidic portion of the stomach without disintegrating, before breaking down only in the small intestine.
A good example of this is omeprazole, a common medication for acid reflux AKA heartburn. Despite omeprazole reducing acid in the stomach, it is acid labile and would get destroyed if exposed to stomach acid before it reaches the intestine. Hence an enteric coating is required for omeprazole to reach the small intestine for absorption and retain its efficacy. This is why omeprazole packaging comes with do not crush or chew labels, as that can destroy the enteric coating.
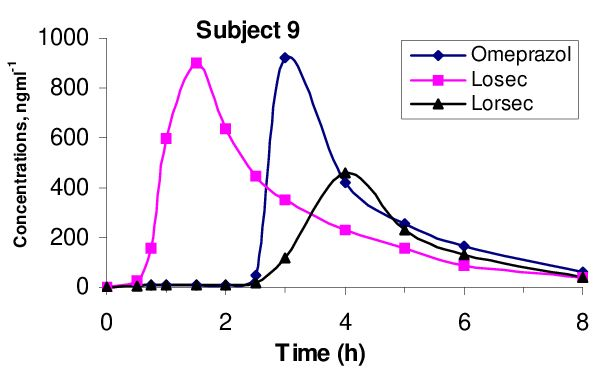
The enteric coating can change the drug’s concentration-time profile too. As the tablet only disintegrates in the small intestine instead of the stomach, this reflects as a lag time before we start detecting drug being absorbed into the blood. Depending on the type of formulation, the rate of release of omeprazole may also differ and impact the overall absorption rate of the drug. (see attached figure from Mostafavi SA et al. https://www.researchgate.net/publication/286716167_Relative_bioavailability_of_omeprazole_capsules_after_oral_dosing#fullTextFileContent) We can use either a transit or a lag compartment to model this delay in absorption. This allows us to capture the actual absorption process, while accounting for the effect of the enteric coating.
For those interested, there are differences between choosing a lag versus a transit compartment. You can read more about it here. https://www.page-meeting.org/page/page2004/savic.pdf Ultimately, I generally go with the choice that describes the data the best.